by Odile A. van den Heuvel, MD, PhD, Chris Vriend, PhD, Nadza Dzinalija, MSc, H. Blair Simpson, MD, PhD, Ilya M. Veer, PhD, Henrik Walter, MD, PhD, Iliyan Ivanov, MD, Paul M. Thompson, PhD, and Dan J. Stein, MD, PhD.
This article was initially published in the Spring 2022 edition of the OCD Newsletter.
Background of the ENIGMA-OCD Consortium
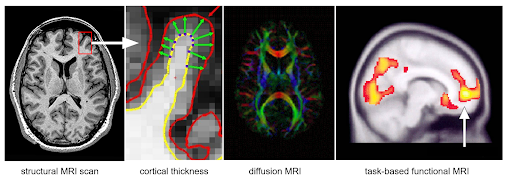
Brain imaging is a powerful tool that has greatly contributed to our understanding of mental health disorders, including obsessive-compulsive disorder (OCD). Since the 1980s, researchers worldwide have extensively used brain imaging techniques to study the structure and function of the brain in people with OCD compared to people without OCD. This research has pointed to specific brain structures and patterns of brain activity (in specific brain circuits) that may be involved in OCD symptoms and has suggested ways to target brain circuits with treatment approaches including medication, psychotherapy, and neurostimulation (e.g., deep brain stimulation or transcranial magnetic stimulation) (Stein et al., 2019). Currently, magnetic resonance imaging (MRI, see Figure 1) is the most used brain imaging technique. With structural MRI it is possible to study the size and shape of the different structures and regions of the brain. With “diffusion MRI” we can visualize the white matter tracts (the highways in the brain) that connect the superficial and deep structures. With a technique called functional MRI (fMRI), it is possible to observe a “live” picture of brain activity as it is triggered by various situations and experiences (for example, the areas of the brain are most active when OCD symptoms are triggered).
MRI and fMRI are powerful tools for advancing our understanding of OCD as well as developing new treatment targeting specific brain circuits. However, brain imaging research has some serious limitations. The time it takes to collect data from participants and the enormous cost of MRI equipment are critical barriers. As a result, most imaging studies in OCD are rather small and limited to strictly defined groups. This limits the “statistical power” of brain imaging studies, making it more difficult for researchers to draw conclusions about whether the differences they see in the brains of people with OCD are real causes and consequences of OCD or are just due to random variations that happen from person to person.
To better understand why statistical power is so important, consider what happens when you step outside on a day when the temperature is much colder than it was the day before. You don’t need a thermometer to know that it is colder outside than it was yesterday — the temperature change is so great that it’s obvious to you just from the way the air feels on your skin. But what if the temperature had only changed by one or two degrees instead? In this case, you may not be able to tell that it’s changed at all. A research study with low statistical power is just like this. It may be able to find big differences between groups, but it will not be able to draw conclusions about small changes with any real confidence. Now, consider the example above, but this time you have a digital thermometer with you when you step outside. The thermometer is sensitive enough to detect small changes in temperature. This is like a study with high statistical power. Statistical power doesn’t just come from the accuracy of the tools available to researchers, but also from the number of participants who they are able to include in their research. Since MRI is not a very sensitive tool and the alterations in OCD are small and dependent on multiple variables, in imaging research we need big samples to get reliable results.
The first large MRI study of OCD focused on detecting physical differences in the brain's structures included data from a single research center (Pujol et al., 2004). A total of 72 people with OCD and 72 healthy individuals (controls) participated. This study found that some regions of the brain were smaller or bigger in people with OCD when compared to participants in the healthy control group. People with OCD had, on average, smaller prefrontal regions (areas relevant for emotional processing, located near the forehead) and larger striatum (a set of regions deep within the brain known to be involved in repetitive behaviors). Research studies that analyzed data from the results of multiple, independent MRI studies in OCD were subsequently published (e.g., Radua et al., 2009). These studies used statistical methods to estimate the overall degree of difference between people with and without OCD. The first study in which researchers pooled and analyzed raw MRI data from multiple sites around the world was performed by the OCD Brain Imaging Consortium (OBIC) — the initial attempt to bring OCD scientists together to work on brain imaging data that they had already independently collected (de Wit et al. 2014).
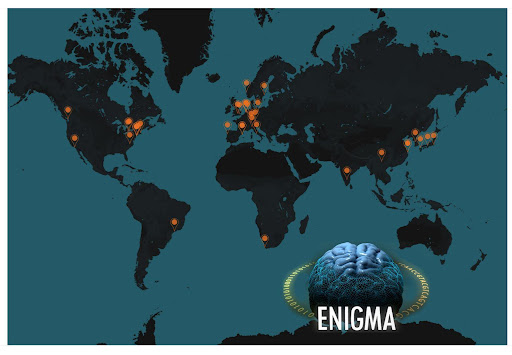
In 2009, Paul Thompson and colleagues initiated the ENIGMA (Enhancing Neuroimaging and Genetics through Meta-analysis) consortium, which has grown to include more than 2,000 scientists from 45 countries who study the human brain in health and disease (Thompson et al., 2020, 2022). The initial aim was to perform large-scale imaging and genetics research by pooling worldwide data, resources, and expertise; and to answer clinical and fundamental questions related to psychiatric and neurological disorders. Now the consortium has more than 50 working groups that focus on 1) specific psychiatric and neurological disorders, 2) trans-diagnostic constructs (e.g., suicidality, lifespan), and 3) the development of analysis pipelines to make it easier to harmonize data across different working groups. Harmonization ensures that data collected at different sites around the world is used and analyzed with a consistent set of techniques, allowing researchers to make “apples to apples” comparisons, even when data has been collected by different research teams at sites many thousands of kilometers apart.
In 2013, Odile van den Heuvel, MD, PhD and Dan Stein, PhD initiated the ENIGMA-OCD working group by bringing in OBIC and inviting new members to contribute. As of 2021, ENIGMA-OCD consists of data from 48 cohorts of research participants from 36 institutes in 15 countries on five continents, with a total sample of 4,669 with MRI data of 2,334 OCD patients (1,835 adults (>18 years), 359 adolescents (12-17 years), 140 children (<12 years)) and 2,335 healthy controls (1,734 adults, 325 adolescents, 166 children). The ENIGMA-OCD consortium is the largest worldwide collaboration on brain imaging in OCD and, with a large set of high-quality imaging data from so many research participants around the world, is able to analyze imaging results with high statistical power in a cost-efficient way. New members are continuously welcomed, and with an open structure, ENIGMA-OCD represents a unique and highly productive example of team science (see Figure 2).
First Findings on Brain Structure in OCD
We recently summarized the findings of the first five years of ENIGMA-OCD in a review paper (van den Heuvel et al. 2022). The first analyses of the ENIGMA-OCD consortium focused on the size of brain regions deep within the brain, such as the thalamus (Boedhoe et al. 2017). We found clear differences between children and adults with OCD: pediatric OCD was associated with a larger thalamus, but this was only detectable when comparing unmedicated children with OCD to healthy children (differences between medicated children with OCD and healthy controls were not detectable). We recently replicated this finding with data from the Generation R cohort in the Netherlands, in which children with probable OCD (scoring above the cut-off on the short OCD screener) also had a larger thalamus (Weeland et al. 2020). This may suggest that the brain develops differently in children prone to develop OCD. Adults with OCD on average had a smaller hippocampus (a part of the brain important to forming long-term and visual memories), and this difference was more obvious in patients with comorbid depression. A smaller hippocampus has also been reported by the ENIGMA working groups for schizophrenia, bipolar disorder, major depressive disorder, and posttraumatic stress disorder, and so may be related to the chronic distress that is present in all these disorders. We also observed that adults with childhood onset OCD were more likely to have a larger pallidum (a part of the brain that helps regulate voluntary motor movement), possibly due to chronic engagement in compulsions or medication use.
The second analysis focused on the cortex, which is the outermost layer of the brain. We showed that people with OCD (both children and adults) have a thinner bilateral inferior parietal cortex, a part of the cortex located near the temples that’s responsible for a range of brain functions, including interpreting sensations or experiences (Boedhoe et al. 2018). Whether or not a patient was taking medication had a strong effect on the findings: compared to healthy controls, children with OCD using medication showed widespread surface area differences (mainly in regions at the front of the brain) and medicated adults with OCD had a thinner cortex, especially in regions near the forehead, temples, and back of the head (frontal, temporal, parietal, and occipital regions). In contrast, unmedicated children and adults with OCD did not differ from controls in the thickness and surface area of the cortex. These medication effects should be interpreted with caution because the study represents a snapshot in time, rather than a long-term study that tracks changes over the course of medication use. However, what we found suggests that medication can physically change the brain and reorganize the ways in which it functions in both children and adults.
Importantly, although the differences we observed between the brains of healthy individuals and people with OCD were often subtle, the increase in statistical power achieved through the ENIGMA-OCD collaboration made it clear that these changes were both real and linked to OCD in some way.
After completing research on the sizes of different brain structures in OCD, we began investigating how these structures were physically interconnected with one another. We analyzed data from studies that used imaging techniques that reveal the physical networks that exist in the brain (Yun et al., 2020; Piras et al., 2021). These networks can tell us important information about how the brain is developing and maturing and are of great interest to researchers studying disorders like OCD that affect brain development and have chronic symptoms over the course of a person's life. Our findings showed that individual networks in the brain were less compartmentalized and more interconnected in OCD than in healthy individuals, and that the distribution of central network “hubs” was different in OCD (Yun et al. 2020). We also found that these differences in OCD were associated with how old an individual was when they developed OCD and how long they had had the disorder, leading us to believe that these changes are more likely a consequence of having OCD than the cause of the disorder itself (Piras et al., 2021).
To summarize, the ENIGMA-OCD consortium has demonstrated the power of global collaboration. By combining already collected structural imaging data, we have shown that some alterations in brain structure in OCD patients likely arise as the brain develops in childhood and adolescence, and that other changes are likely due to the effects of having a chronic mental health disorder for many years, and still others may result from medication use. These findings have important consequences. First, they highlight the importance of conducting long-term studies that examine and track the effects of medication on the developing brain over time. Second, they underscore the urgent need to intervene early and reduce the amount of time that it takes to begin effective treatment after the first symptoms of OCD set in (e.g., by increasing access to exposure and response prevention [ERP] treatment across the globe). The need to prevent OCD from altering the brain is critical and must be accomplished by connecting people to evidence-based treatment early on, as well as by developing innovative treatments for those who do not respond to existing first-line interventions like ERP and medication.
Project on Brain Function Funded by the 2021 IOCDF Innovator Award
In 2021, the International OCD Foundation (IOCDF) awarded a $300,000 research grant (the Innovator Award) to the ENIGMA-OCD consortium (PIs: Odile van den Heuvel, MD, PhD and Chris Vriend, PhD), to support the next stage of worldwide collaboration. In this project, we will investigate brain function in OCD and study the connections between brain function and our previous findings about the brain’s structure. We will use functional MRI (fMRI) scans to study the brain activity of participants during specific cognitive and emotional tasks.
Task-based fMRI has greatly advanced our understanding of how the brains of people with OCD work differently from healthy individuals; however, previous task-based fMRI studies were limited by small samples. In the IOCDF Innovator Award project, we will bring together fMRI data from sites around the world to increase the statistical power of our research on brain activity in OCD. Our research will focus on emotional processing, the processes that enable individuals to resist engaging in compulsions, and higher-order thinking processes that enable people to interpret and respond to the world around them (see figure 3). We will address three crucial questions: 1) How does obsessive and compulsive behavior shape the brain? 2) How does medication used to treat OCD alter brain function? 3) Can brain function predict an individual’s treatment response?
First, we expect that people with OCD will show different brain activation when compared to healthy controls during tasks that tap into patterns of thinking and emotional processing that underlie OCD symptoms, and that these differences will depend on age (stage of brain development) and disease duration (how long a person has had OCD). Second, we expect that brain activity will differ between people with OCD who use medication as compared to those without medication. Third, we expect that some patterns of brain activity in OCD will be linked to better response to ERP and serotonin reuptake inhibitor medications. In particular, we believe that individuals who have more activity in the amygdala (involved in memory, emotional processing, and fear and anxiety responses) and dorsal prefrontal areas (involved in working memory and planning) when processing emotions will respond better to these treatments.
To conclude, ENIGMA-OCD has brought together OCD experts from all over the world to re-analyze historical MRI data using a range of statistical methods, increasing the statistical power of OCD brain imaging research and improving our ability to make important discoveries about this disorder using MRI. The IOCDF Innovator Award will bring this research to the next level by enabling us to study brain function with the same approach. Our ultimate goal is to translate knowledge on brain structure and function involved in the causes and consequences of OCD, leading to better outcomes for people living with OCD.
References
Boedhoe, P.S.W., Schmaal, L., Abe, Y., …, van den Heuvel, O.A. (2017). Distinct subcortical volume alterations in pediatric and adult OCD; a worldwide meta- and mega-analysis. The American Journal of Psychiatry, 174, 60-70.
Boedhoe, P.S.W., Schmaal, L., Abe, Y., …, van den Heuvel, O.A. (2018). Cortical abnormalities associated with pediatric and adult obsessive-compulsive disorder: findings from the ENIGMA Obsessive-Compulsive Disorder working group. The American Journal of Psychiatry, 175, 453-462.
De Wit, S.J., Alonso, P., Schweren, L., …, van den Heuvel, O.A. (2014). Multi-center voxel-based morphometry mega-analysis of structural brain scans in obsessive-compulsive disorder. The American Journal of Psychiatry, 171, 340-349.
Piras, F., Piras, F., Abe, Y., …, Spalletta, G. (2019). White matter microstructure and its relation to clinical features of obsessive-compulsive disorder: findings from the ENIGMA OCD Working Group. Translational Psychiatry 2021, 11, 173. doi: 10.1038/s41398-021-01276-z
Pujol, J., Soriano-Mas, C., Alonso, P., ..., Vallejo, J. (2004). Mapping structural brain alterations in obsessive-compulsive disorder. Archives of General Psychiatry, 61, 720-30.
Radua, J., Mataix-Cols, D. (2009). Voxel-wise meta-analysis of grey matter changes in obsessive-compulsive disorder. British Journal of Psychiatry, 195, 393-402.
Stein, D.J., Costa, D.L.C., Lochner, C., …, Simpson, H.B. (2019). Obsessive-compulsive disorder. Nature Reviews Disease Primers, 5, 52.
Thompson, P.M., Jahanshad, N., Ching, C.R.K., …, Zelman, V. (2019). ENIGMA and global neuroscience: a decade of large-scale studies of the brain in health and disease across more than 40 countries. Translational Psychiatry, 2020, 10, 100.
Thompson, P.M., Jahanshad, N., Schmaal, L., …, Kochunov, P. The Enhancing Neuroimaging Genetics through Meta-analysis Consortium: 10 years of global collaborations in human brain mapping. Human Brain Mapping, 2022, 43, 15-22.
van den Heuvel, O.A., van Wingen, G., Soriano-Mas, C., …, Veltman, D.J. (2016). Brain circuitry of compulsivity. European Neuropsychopharmacology, 26, 810-27.
Van den Heuvel, O. A., Boedhoe, P. S., Bertolin, S., Bruin, W. B., Francks, C., Ivanov, I., ... & Yamada, K. (2022). An overview of the first 5 years of the ENIGMA obsessive–compulsive disorder working group: The power of worldwide collaboration. Human Brain Mapping, 43(1), 23-36.
Yun, J.Y., Boedhoe, P.S.W., Vriend, C., …, Kwon, J.S. (2019). Brain structural covariance networks in obsessive-compulsive disorder: a graph analysis from the ENIGMA consortium. Brain, 2020, 143, 684-700.