Medication Treatment for Obsessive Compulsive Disorder in Adults
by Steven Poskar, MD
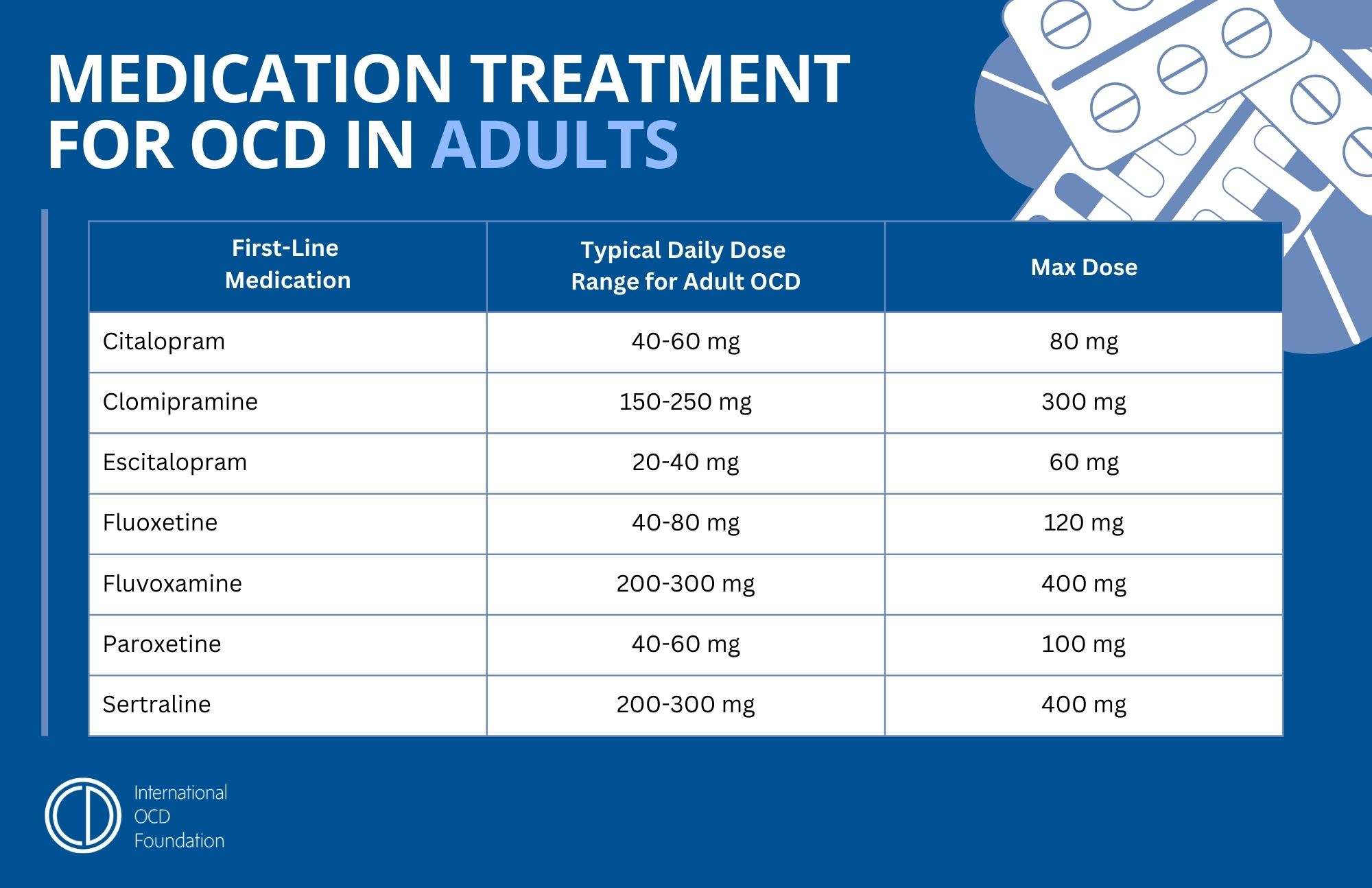
Selective Serotonin Reuptake Inhibitors (SSRIs) are the first-line medications for OCD. SSRIs and Clomipramine are the only medications found to be effective standalone treatments for OCD. The SSRIs include Citalopram (Celexa), Escitalopram (Lexapro), Fluoxetine (Prozac), Fluvoxamine (Luvox), Paroxetine (Paxil), and Sertraline (Zoloft).
With any given trial of an SSRI, about 40-60% of patients with OCD will have a clinically significant improvement in OCD symptoms and overall functioning. For those who respond, the average degree of improvement is a 40-50% decrease in the severity of OCD symptoms.
Augmentation of an SSRI or Clomipramine with an Adjunctive Medication
Adjunctive Antipsychotics
The most common, and most evidenced-based, augmentation strategy is to add low-dose Dopamine Type 2 (D2) Receptor Antagonists (Blockers). These medications are known as antipsychotics because they were first developed and used to treat psychosis. This name persists even though these medications are now more often used for a myriad of conditions outside of psychosis.
When used to augment SSRIs in the treatment of OCD, the doses used are lower than those typically used for schizophrenia and bipolar disorder. Approximately one-third of patients who do not have satisfactory responses to an SSRI alone will respond when a low-dose D2 Receptor Antagonist is added.
There are multiple D2 Receptor Antagonists, but clinicians have the most evidence to support the newer, atypical antipsychotics, Aripiprazole and Risperidone. There is also some evidence to support the use of adjunctive Olanzapine or Quetiapine, or low-dose Haloperidol, one of the older, first-generation antipsychotics. However, those medications have a higher rate of short-term and long-term side effects.
Using antipsychotics on their own, without an SSRI, is not effective for OCD. Furthermore, the newer atypical antipsychotics, when used alone, can worsen or produce OCD symptoms - usually in people with schizophrenia or bipolar disorder.
Adjunctive Clomipramine
Another common augmentation strategy is augmenting an SSRI with Clomipramine. The logic here is that a patient may get the benefit of the SSRI and Clomipramine, while using lower doses of Clomipramine than required when using it alone, thereby minimizing the side effects associated with higher doses of Clomipramine. Studies have found this combination to be effective.
Adjunctive Glutamate Modulators
One important brain abnormality that is thought to underlie OCD in some patients is elevated activity of the neurotransmitter glutamate in the brain circuits that mediate OCD symptoms. This has led to promising research on various medications that modulate glutamate in different ways, including some anticonvulsants, such as lamotrigine and topiramate. No large-scale definitive studies have been conducted on these agents as of the time of this writing, but several smaller randomized, placebo-controlled studies and open trials have found some of these medications to be effective adjuncts to SSRIs for treatment-refractory OCD.
While there is less data on using glutamate modulators to augment SSRIs for OCD than there is for low-dose antipsychotic augmentation, there are instances when using glutamate modulators to augment SSRIs for OCD may be tried prior to low-dose antipsychotics, because glutamate modulators typically have better side-effect profiles. The glutamate modulators that are the most well studied as SSRI augmenters for OCD are Memantine, N-Acetylcysteine, Lamotrigine, Topiramate, Riluzole, and Ketamine.
Adjunctive Serotonin-3 Receptor Antagonists
Serotonin-3 receptor antagonists such as Ondansetron and Granisetron are commonly used for treatment of nausea and gastrointestinal disorders. However, numerous randomized, placebo-controlled studies and open trials have found that adding Ondansetron or Granisetron to an SRI is effective for treatment of OCD in individuals who did not have adequate response to SRIs alone.